AI Clinical Scribe
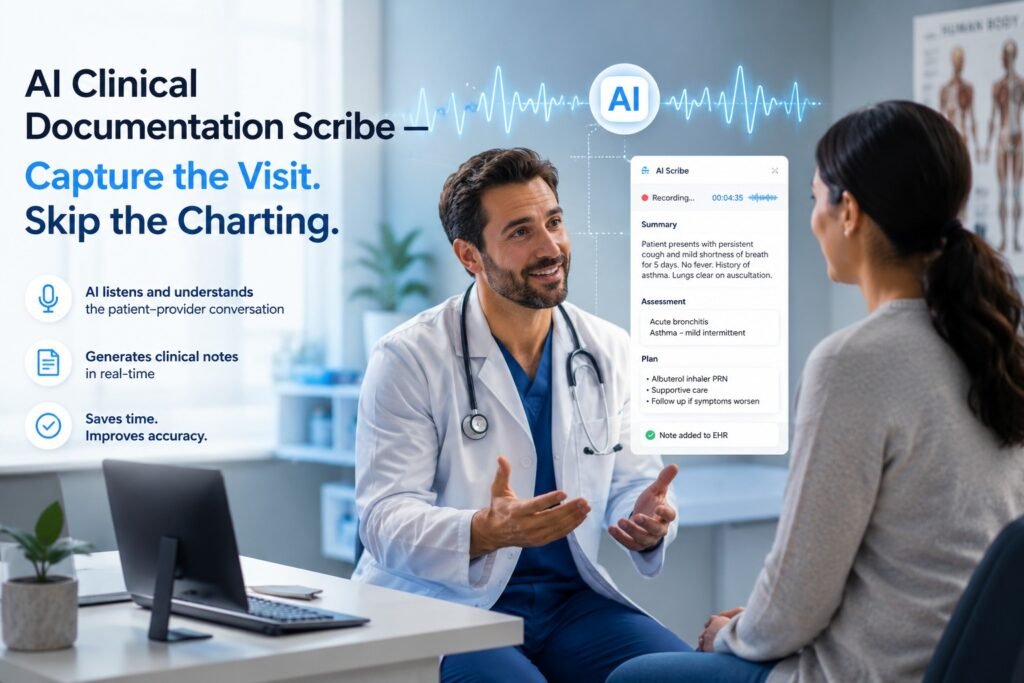
AI Clinical Documentation Scribe — Capture the Visit.
Skip the Charting.
The average physician spends nearly 50% of their workday on documentation — and another two hours every evening on “pajama-time” charting. That is time stolen from patients, from sleep, and from the medicine you trained a decade to practice. The MedCods AI Clinical Documentation Scribe listens passively during your patient encounter and generates a structured, specialty-specific clinical note within seconds — pre-mapped to ICD-10 and CPT codes, ready for your review and signature. Unlike standalone scribe apps, MedCods feeds the note directly into the same platform that handles your coding, claim submission, and revenue cycle — so the encounter that produced the note is the same one that gets billed cleanly, on the first pass.
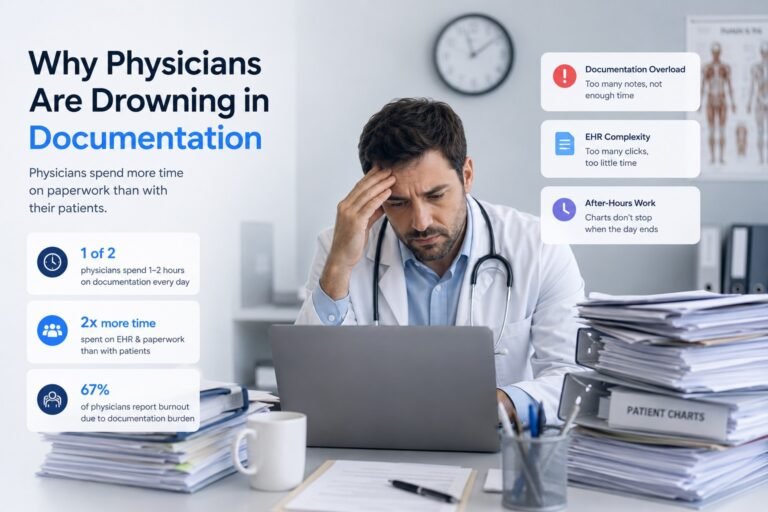
Why Physicians Are Drowning in Documentation
Clinical documentation has not always been this heavy. EHR adoption mandates, MIPS quality reporting, payer documentation requirements, and risk-adjustment coding have each added a layer to the chart over the last fifteen years. The result: physicians now type more than they examine, click more than they think, and finish notes long after the patient has gone home.
The financial cost is measurable. Late or thin documentation directly drives claim denials, downcoding, and lost revenue — a single under-documented E/M encounter can cost a practice $30 to $90 in collected reimbursement. The personal cost is worse. According to multiple peerreviewed studies published in 2025 and 2026, documentation burden is one of the top three
drivers of physician burnout. A 2025 survey of small primary care practices found a 60% reduction in burnout after adopting an ambient AI scribe. The Permanente Medical Group reported 15,791 documentation hours saved across 7,260 physicians in a single year.
The conclusion across the literature is consistent: clinical documentation done by a clinician at the keyboard is the most expensive, lowest-value use of physician time in modern medicine. Ambient AI scribes change that arithmetic.
How the MedCods AI Clinical Scribe Works
Stage 01
Ambient Capture in the Exam Room
Open the MedCods app on your phone, tablet, or computer. Tap Record at the start of the encounter. The scribe listens in the background — no special microphones, no structured dictation, no scripted phrasing required. You speak naturally with your patient. The patient speaks naturally with you. The MedCods Scribe distinguishes speakers, captures medical context, and ignores small talk.
Stage 02
Structured Note Generation in Seconds
The moment you tap End Recording, the MedCods Scribe generates a fully structured clinical note — typically in under one minute. SOAP, DAP, or specialty-specific formats are supported. ICD-10 and CPT code suggestions are pre-populated based on the documented encounter. HPI, ROS, exam findings, assessment, plan, and risk-stratification language are all generated from the conversation — not from a template you have to fill in.
Stage 03
Clinician Review and Specialty Templating
Every note is presented for your review before it touches the chart. You remain the legal and clinical author of the documentation. The MedCods Scribe supports 30+ specialty templates — including cardiology, behavioral health, orthopedics, OB/GYN, dermatology, pediatrics, family practice, and more — so the structure of your note matches how your specialty actually documents care.
Stage 04
Direct Integration With Billing and Claims
This is the MedCods difference. The reviewed and signed note is not just dropped into your EHR — it flows directly into the MedCods billing platform. The suggested ICD-10 and CPT codes are validated by the MAXIMUS AI Engine against 3 million+ payer rules before charge entry. Documentation gaps that would trigger denials are flagged for resolution while the patient is still in the building, not 45 days later when the claim comes back rejected.
Core Features of the MedCods AI Clinical Scribe
Ambient Audio Capture, Any Device
Works on phone, tablet, laptop, or desktop. No special microphones, no required hardware. Supports in-person and telehealth visits across continuous sessions up to 90 minutes.
Structured Note Generation in Under 60 Seconds
OAP, DAP, or specialty-specific note formats generated from natural conversation. ICD-10 and CPT code suggestions included automatically.
30+ Specialty Note Templates
Pre-built for cardiology, behavioral health, orthopedics, pediatrics, family practice, OB/GYN, dermatology, pulmonology, endocrinology, oncology, and more — so structure matches your specialty's conventions, not a generic SOAP shell.
Multilingual Conversation Support
Captures English, Spanish, and major additional languages with automatic detection. Generates English notes regardless of conversation language — critical for diverse patient populations.
Speaker Diarization and Context Awareness
Distinguishes clinician, patient, family members, and translators. Ignores non-clinical small talk. Captures medication names, allergies, symptom timelines, and family history precisely.
Native Billing Integration
Notes feed directly into the MedCods billing platform. ICD-10 and CPT suggestions are validated against the MAXIMUS Engine's 3M+ payer rules before charge entry. Documentation gaps caught in real time — not after denial.
40+ EHR Integrations
Direct integration with Epic, Cerner, Athenahealth, AdvancedMD, Kareo/Tebra, Meditech, and 35+ others via HL7, FHIR, and direct API. Notes write back to the patient chart without manual copy-paste.
HIPAA-Grade Security and BAA Included
SOC 2 Type II audited, AES-256 encrypted, audio discarded after note generation (no audio retention by default), and a Business Associate Agreement executed with every client. PHI never used for model training.
Clinician-Controlled Review and Signature
Every note is presented for clinician review before chart submission. The MedCods Scribe is a documentation support tool — the clinician remains the legal and clinical author of every record.
Who Benefits Most from the MedCod AI Scribe
While every clinician benefits from reclaimed documentation time, certain specialties see disproportionate impact. Mental and behavioral health providers, whose 50-minute therapy sessions historically required 15–20 minutes of post-session notes, often gain back two full hours per day. Primary care and family practice physicians, who see 20+ patients daily with high documentation density per encounter, typically reclaim 60–90 minutes per workday. Cardiology, OB/GYN, pediatrics, and orthopedics — all specialties with complex encounter narratives and detailed exam findings — benefit from specialty-templated notes that capture nuance generic
scribes miss.
For multi-provider groups, the impact compounds. A 10-provider practice that recovers an average of 60 minutes of documentation time per clinician per day reclaims roughly 200 hours of physician time per month — time that goes back into patient care, additional appointments, or simply going home before dinner. Recent peer-reviewed research, including a 2026 UCSF / Mass General Brigham JAMA multisite study, found that high-utilization AI scribe users see three times the documentation time reduction compared with light users — making consistent adoption across your providers a meaningful financial and clinical lever.

MedCods AI Scribe vs. Standalone AI Scribe Apps
| CAPABILITY | STANDALONE SCRIBE APPS | MEDCODS AI SCRIBE |
|---|---|---|
| Ambient note generation | ✓ | ✓ Under 60 seconds |
| Specialty-specific templates | Limited / generic | ✓ 30+ templates |
| Multilingual capture | Often English-only | ✓ Multi-language, English output |
| ICD-10 / CPT code suggestion | Basic list | ✓ MAXIMUS-validated, 3M+ rules |
| Documentation gap detection | ✗ Not available | ✓ Real-time, before claim creation |
| Billing platform integration | ✗ Separate tool | ✓ Native, flows into charge entry |
| EHR write-back | Manual copy-paste | ✓ Direct API, 40+ EHRs |
| Audio retention policy | Often retained | ✓ Discarded after note generation |
| Business Associate Agreement | Sometimes negotiated | ✓ Standard with every client |
| Per-provider monthly cost | $59–$199/clinician | ✓ Included in MedCods RCM pricing |
The Financial and Clinical Impact
Documentation time recovered
Practices using the MedCods AI Scribe with high consistency (more than 50% of visits) report time reductions in the range documented by recent JAMA and JMIR studies — often 30–60 minutes per provider per day in active practice, with heavy users seeing the highest gains.
Burnout reduction
A 2025 survey of small primary-care practices reported a 60% reduction in self-reported burnout within 90 days of ambient scribe adoption. A 2025 Yale study documented measurable burnout score reductions in just 30 days.
Revenue capture improvement
Specialty-templated notes with MAXIMUS-validated CPT and ICD-10 suggestions reduce the documentation gaps that drive downcoding and denial. UCSF's 2025 JAMA Network Open study found AI scribe users generated an average of $3,044 more revenue per year and saw 0.8 more patients per week than non-users.
Patient experience improvement
When the clinician is not behind a keyboard for half the visit, eye contact and conversational engagement measurably improve — multiple time-motion studies have documented eye-contact increases of 7% or more during AI-scribed visits.
Compliance posture strengthened
Audio discarded by default, BAA executed standard, AES256 encryption, and a Security Risk Analysis already conducted on the platform — closing the most common compliance gaps that AI scribe vendors leave open.
FrequentlyAsked Questions — AI Clinical Documentation Scribe
Q: How accurate is the MedCods AI Clinical Scribe in real clinical environments?
The MedCods AI Scribe achieves clinical-grade transcription accuracy across real-world environments — including background noise, multi-speaker conversations, and accented speech. That said, no AI scribe is 100% accurate, and the literature is clear on this point. Every note is presented for clinician review and signature before it enters the patient chart. The clinician remains the legal and clinical author of the documentation, and the MedCods Scribe functions as a documentation support tool — not a replacement for clinical judgment.
Q:Is the MedCods AI Scribe HIPAA compliant? What about audio recordings of patient encounters?
Yes. The MedCods AI Scribe is fully HIPAA compliant, SOC 2 Type II audited, and uses AES-256 encryption for all data at rest and in transit. By default, audio recordings are discarded immediately after the structured clinical note is generated — meaning the only retained data is the clinical note itself, governed by the same policies as any other EHR record. We execute a Business Associate Agreement (BAA) with every client as a standard part of onboarding, and PHI is never used to train models.
Q: Do I need patient consent to use the MedCods AI Scribe during visits?
Best practice — and a requirement in many U.S. states — is to inform patients that an AI documentation tool is being used and to give them the option to opt out. MedCods provides standard patient notice language, consent workflows, and signage that practices can deploy at the front desk. State audio-recording laws vary, and your compliance officer should review the consent workflow against the requirements of every state in which your practice operates.
Q: Does the MedCods AI Scribe integrate with my EHR?
Yes. MedCods integrates with more than 40 EHR systems — including Epic, Cerner, Athenahealth, AdvancedMD, Kareo/Tebra, and Meditech — via HL7, FHIR, and direct API
connections. Reviewed and signed notes write back into the patient chart automatically. There is no manual copy-paste step.
Q: What specialties does the MedCods AI Scribe support?
MedCods supports 30+ specialties, including cardiology, mental and behavioral health, orthopedics, pediatrics, family practice, OB/GYN, dermatology, pulmonology, endocrinology, oncology, radiology, and more. Each specialty carries pre-built note templates aligned to how that specialty actually documents care — not retrofitted from a generic SOAP shell.
Q:Is the MedCods AI Scribe regulated as a medical device by the FDA?
Ambient AI scribes that assist with documentation — and do not diagnose, treat, or make clinical decisions — have generally not been treated as FDA-regulated medical devices. The MedCods AI Scribe operates as a documentation support tool. The clinician reviews and signs every note, and clinical decision-making remains with the clinician. This is consistent with current regulatory guidance and industry practice for ambient documentation tools.
Q: How is the MedCods AI Scribe priced?
The MedCods AI Scribe is included in the MedCods Full RCM Platform — not billed separately on a per-provider, per-month basis. That means practices on the MedCods RCM platform get unlimited AI scribe usage across all providers at no additional cost. For practices that need only the AI Scribe without full RCM, a per-provider monthly plan is available. Either way, there are no setup fees and no long-term contracts.
Start Within 72 Hours
Documentation Shouldn't Keep
You Up Until 9 p.m.
Ambient capture that respects your patient conversation, specialty-templated notes in seconds, and direct billing integration — all inside the same MedCods platform that handles your revenue cycle.